PTOSIS.
In blepharoptosis, the upper eyelid droops below its normal level.
Congenital ptosis is usually a result of a localized dystrophy of the levator
muscle in which the striated muscle fibers are replaced with fibrous tissue.
The condition may be unilateral or bilateral and can be familial, transmitted
as a dominant trait.
Parents often comment that the eye looks smaller because of the drooping eyelid. The lid crease is decreased or absent where the levator muscle would normally insert below the skin surface. Because the levator is replaced by fibrous tissue, the lid does not move downward fully in downgaze (lid lag). If the ptosis is severe, affected children often attempt to raise the lid by lifting their brow or adapting a chin-up head posture to maintain binocular vision. Marcus Gunn jaw-winking ptosis accounts for 5% of ptosis in children. In this syndrome, an abnormal synkinesis exists between the fifth and third cranial nerves; this causes the eyelid to elevate with movement of the jaw. The wink is produced by chewing or sucking and may be more noticeable than the ptosis itself.
Although ptosis in children is often an isolated finding, it may occur in association with other ocular or systemic disorders. Systemic disorders include myasthenia gravis, muscular dystrophy, and botulism. Ocular disorders include mechanical ptosis secondary to lid tumors, blepharophimosis syndrome, congenital fibrosis syndrome, combined levator/superior rectus maldevelopment, and congenital or acquired 3rd nerve palsy. A complete ophthalmic and systemic examination is therefore important in the evaluation of a child with ptosis.
Amblyopia may occur in children with ptosis. The amblyopia may be secondary to the lid's covering the visual axis (deprivation) or induced astigmatisim due to the weight of the lid on the globe (anisometropia). When amblyopia occurs, it should generally be treated before treating the ptosis.
Treatment of ptosis in a child is indicated for elimination of an abnormal
head posture, improvement in the visual field, prevention of amblyopia,
and restoration of a normal eyelid appearance. The timing of surgery depends
on the degree of ptosis, its cosmetic and functional severity, the presence
or absence of compensatory posturing, the wishes of the parents, and the
discretion of the surgeon. Surgical treatment is determined by the amount
of levator function that is present. A levator resection may be used in
children with moderate to good function. In patients with poor or absent
function, a frontalis suspension procedure may be necessary. This technique
requires that a suspension material be placed between the frontalis muscle
and the tarsus of the eyelid. It allows patients to use their brow and
frontalis muscle more effectively to raise their eyelid. Amblyopia remains
a concern even after surgical correction and should be monitored closely.
Yanoff: Ophthalmology, First Edition, Copyright ©
1999 Mosby International Ltd.
--------------------------------------------------------------------------------
--------------------------------------------------------------------------------
Section 7
5 . 1
Chapter 5 - EYELIDS - Blepharoptosis
--------------------------------------------------------------------------------
Philip L Custer
--------------------------------------------------------------------------------
INTRODUCTION
Blepharoptosis (ptosis) results from congenital or acquired abnormalities
of the levator or Muller's neuromuscular complexes. It can be defined as
an abnormally low position of the upper eyelid margin, determined while
the eye is looking in primary gaze. Trauma and orbital masses may also
cause mechanical ptosis.
Ptosis may present with a variety of symptoms, including superior visual field obstruction, headache, and fatigue. Contact lens patients may report difficulty wearing or inserting their lenses. Ptosis repair is considered in those patients who are symptomatic or displeased with the cosmetic appearance of their eyelid. It is the goal of ptosis repair to adequately elevate the eyelid, while minimizing the risks of lagophthalmos and ocular exposure.
HISTORICAL REVIEW
Surgeons prior to the mid-1800s repaired blepharoptosis by excising
upper eyelid skin, essentially suspending the eyelid from the brow. The
frontalis suspension was popularized in the nineteenth century when physicians
utilized a variety of subcutaneous implants to create a direct connection
between the drooping eyelid and the forehead. Sutures, wires, xenografts,
and autologous tissue grafts were employed. Motais and Parinaud introduced
the superior rectus suspension procedure in 1897 [1] [2] . A portion of
the superior rectus muscle was transposed and attached to the eyelid. Unfortunately,
the resulting adhesion limited the independent movement of the eyelid and
globe, compromising eyelid closure and blinking. Enthusiasm for this procedure
declined as patients developed complications from chronic ocular exposure.
Bowman (1857) is credited with the first description of a procedure to shorten the levator-Muller's muscle complex through a conjunctival (posterior) incision [3] . An anterior levator technique was subsequently reported in 1883 by Eversbusch and Snellen [4] [5] . In 1975, Jones et al. determined that many cases of acquired ptosis were caused by a dehiscence of the levator aponeurosis. They described a technique to repair this structure that successfully elevated the eyelid [6] .
Modern physicians use a variety of ptosis procedures, depending upon the levator muscle function (see below). Patients who have poor levator function often require frontalis suspension. Anterior levator aponeurotic shortening is widely employed in patients who have good levator activity. Some surgeons prefer a posterior resection of Muller's muscle in these individuals.
PREOPERATIVE EVALUATION AND DIAGNOSTIC APPROACH
The ocular and medical history
The initial evaluation is directed toward determining the cause of
the ptosis. The medical history should ascertain the age of onset, duration,
severity, and variability of the condition. Interviewing family members
and reviewing old photographs are helpful to document the progression of
the disorder. The family history may be revealing in some forms of ptosis
with hereditary patterns. Previous ocular trauma, ocular surgery, or eyelid
disease may have contributed to the development of ptosis or alter the
treatment plan. Ptosis repair should be considered with caution in patients
who have prior symptoms of ocular irritation, dryness, photophobia, or
diplopia. True eyelid ptosis must be differentiated from the various causes
of pseudoptosis including dermatochalasis, contralateral eyelid retraction,
enophthalmos, and hypotropia.
The presence of concomitant ocular signs may help make a diagnosis. Ipsilateral miosis is suggestive of Horner's syndrome, while mydriasis may be found in cases of previous oculomotor paralysis. Patients who have surgically or traumatically enlarged pupils often suffer photophobia, which may worsen following ptosis surgery. Significant ocular inflammation or dryness may be responsible for a reactive ptosis; if present, these conditions must be corrected prior to contemplating ptosis repair. A Schirmer's test should be used to measure the basic tear secretory rate in adult patients. In cases of reduced tear function, surgery should be limited or avoided in order to avoid exacerbation of dry eye syndrome.
Preoperative photographs are obtained to document the severity of ptosis. Visual fields with and without elevation of the drooping eyelids are used to determine the degree of visual obstruction. Additional diagnostic studies, such as orbital imaging or neuromuscular testing, may be indicated when clinical examination fails to determine the cause of the ptosis.
Bell's phenomenon
With eyelid closure, reflex innervation to the extraocular muscles
result in an upward and slightly outward rotation of the globe. This mechanism
protects the cornea in cases of lagophthalmos. In patients who have reduced
or absent Bell's phenomenon, ptosis repair should be conservative to avoid
postoperative exposure problems. This is especially true in patients who
show pre-existing dry eye.
Hering's law
The levator muscles obey Hering's law of equal innervation [7] . Since
the levator muscles are innervated from a single midline nucleus, central
neural output is equal to both levator muscles. Thus, in cases of bilateral
but asymmetric ptosis, the less affected eyelid may be capable of maintaining
a normal level of elevation due to excessive innervational stimulation
determined by the more ptotic eyelid. This condition may be detected prior
to surgery by manual elevation of the ptotic eyelid. An immediate fall
of the contralateral eyelid confirms the presence of bilateral, asymmetric
ptosis masked by levator 'overaction' [8] .
Levator muscle function
Levator muscle function is determined by measuring the excursion of
the eyelid margin as the patient looks from downgaze to upgaze. The eyebrow
must be manually fixed against the supraorbital rim during this measurement
in order to prevent the frontalis muscle from contributing to the eyelid
movement. Many patients subconsciously raise their eyebrow in a compensatory
effort to elevate the drooping lid, a beneficial finding in individuals
who may require frontalis suspension. Normal adults typically demonstrate
13-16mm of levator function [9] . Lesser measurements may indicate the
presence of a developmental or acquired myopathy.
--------------------------------------------------------------------------------
Section 7
5 . 2
Other measurements
The upper eyelid margin is normally positioned 1-2mm below the superior
limbus, well above the pupil. The position of the upper eyelid margin is
measured while the patient looks in primary gaze. This may be recorded
as the position (in millimeters) of the upper eyelid margin below the superior
limbus, or its position (above or below) with respect to the midpupillary
light reflex.
The position of the upper eyelid crease in both eyes is measured and recorded, along with the amount of redundant skin (dermatochalasis). This is important, especially in cases of unilateral ptosis, so that a normal lid crease can be reformed at the time of surgery. Ocular motility must be assessed in all patients who have ptosis. A coexisting strabismus may be detected in some patients who have congenital ptosis, acquired neurologic or myopathic disease, or in the presence of orbital masses. A component of pseudoptosis often is present in cases of hypotropia.
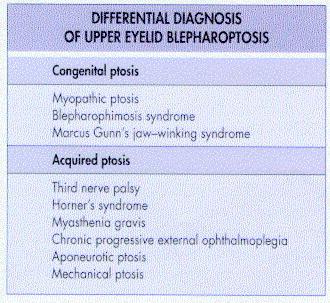
DIFFERENTIAL DIAGNOSIS
Blepharoptosis may be categorized by age of onset, severity, and physiologic
etiology. Ptosis is either congenital or acquired. Mild ptosis may not
be clinically significant, while moderate or severe disease often results
in a cosmetic or functional deficit. A variety of myopathic, neurologic,
and mechanical conditions result in ptosis. The accurate determination
of the cause clarifies the need for ancillary testing, facilitates treatment,
and is of prognostic value. The differential diagnosis of blepharoptosis
is shown in Figure 5.1 .
Congenital ptosis
Simple congenital (myopathic) ptosis
The majority of children who have congenital ptosis suffer from a developmental
myopathy of the levator muscle. This condition is present at birth and
generally remains stable throughout life. Levator muscle function is decreased
in proportion to the severity of the ptosis. The affected levator muscle
is fibrotic, limiting the inferior mobility of the eyelid. The degree of
ptosis usually is less marked in downgaze (Fig. 5.2) . The upper eyelid
crease is typically indistinct or absent. Many children demonstrate compensatory
elevation of their eyebrows or maintain a chin-elevated head position.
Simple congenital ptosis is unilateral in 69% of cases [10] . Bilateral involvement may either be symmetric or asymmetric in appearance. A coexisting ocular motility abnormality is present in approximately 30% of children [11] [12] [13] . Hypotropia is common, a possible manifestation of developmental failure affecting both the superior rectus and levator muscles [14] . Anisometropia is present in 12% of patients with simple congenital ptosis [15] [16] . The ptotic eyelid may cause corneal molding, which results in with-the-rule astigmatism. Strabismus and anisometropia may lead to amblyopia, which is found in 20% of simple congenital ptosis patients [17] . Occlusion amblyopia is less common,
Figure 5-1 Differential diagnosis of upper eyelid blepharoptosis.
remaining a diagnosis of exclusion. Early ptosis repair is indicated in cases with possible occlusion of the visual axis. Surgery is otherwise delayed until the late preschool years.
Children who have good levator function are effectively treated with an anterior levator aponeurotic-muscle resection, while children who have severe ptosis and poor function often require a frontalis suspension. Severe unilateral congenital ptosis remains a treatment challenge. Unilateral frontalis suspension may be considered in children who have compensatory elevation of their eyebrow. Maximal levator resection also can be employed, although this procedure often is complicated by significant postoperative lagophthalmos. Bilateral frontalis suspension combined with ablation of the uninvolved levator muscle provides symmetric eyelid appearance and function. However, most parents are hesitant to consider surgery on the normal eyelid.
Blepharophimosis syndrome
Approximately 6% of children who have congenital ptosis will demonstrate
the typical findings of blepharophimosis syndrome [10] . Severe bilateral
ptosis usually is present with poor levator muscle activity. The palpebral
fissures are horizontally shortened (blepharophimosis) with resultant telecanthus
(Fig. 5.3) . True hypertelorism is occasionally present [18] . Epicanthus
inversus is another common finding. Mild ectropion of the temporal lower
eyelids is seen in severe cases. The inferior puncta often are displaced
laterally and the eyebrows may be abnormally wide. Some patients demonstrate
low-set, 'lop' ears.

Figure 5-2 Simple congenital ptosis. (a) Decreased levator muscle
function occurs along with an indistinct upper eyelid crease. (b) The ptosis
is exaggerated in upgaze due to the poor function of the levator muscle.
(c) In downgaze, the ptosis is reduced or absent because the fibrotic levator
muscle cannot stretch.
--------------------------------------------------------------------------------
Section 7
5 . 3
Blepharophimosis is a dominantly inherited condition, with high penetrance
[19] . The severity of ocular findings may vary among affected family members.
Sporadic cases also may occur. Intelligence is not affected and most patients
who have blepharophimosis are systemically healthy. Blepharophimosis is
associated with primary amenorrhea in some family lines [20] .
Surgical treatment of blepharophimosis usually requires a staged approach. The telecanthus and epicanthal folds often are initially repaired with medial canthal tendon plication and local skin flaps [18] [21] . Bilateral frontalis suspension subsequently is performed to correct the ptosis. Skin grafting may be necessary to relieve coexisting lower eyelid ectropion
Marcus Gunn's jaw-winking syndrome
The jaw-winking syndrome was initially described by Marcus Gunn in
1883 [22] . This form of synkinetic ptosis typically is unilateral and
not hereditary. The ptotic eyelid demonstrates intermittent elevation,
coinciding with contraction of the muscles of mastication (Fig. 5.4) .
The patient is thus noted to 'wink' during eating or chewing. The synkinesis
commonly involves the ipsilateral external pterygoid muscle, which moves
the jaw toward the opposite side. The severity of the ptosis and the amplitude
of the wink are proportionately related. Measurable levator function is
variable or decreased. The upper eyelid crease usually is intact. Hypotropia
and other forms of strabismus may be associated with the jaw-winking syndrome
[23] .
The cause of this condition is unknown, although there appears to be misdirection of either the efferent motor innervation or afferent proprioceptive fibers of the third and fifth cranial nerves [24] [25] . The wink often becomes less noticeable with age, as patients learn to limit oral movements which stimulate the synkinesis [26] . Surgical therapy of the ptosis is challenging. Mild cases can be treated with levator aponeurotic-muscle resection. Patients who have large amplitude winking may require ablation of the levator, followed by frontalis suspension [27] .

Figure 5-3 Blepharophimosis syndrome. (a) With symmetric bilateral
ptosis, telecanthus, and epicanthal folds. (b) Postoperative appearance
following bilateral canthoplasty and frontalis suspension.
Acquired ptosis
Third cranial nerve palsy
The levator muscle is innervated by the superior division of the third
cranial nerve. The levator subnucleus is central and unpaired. Intranuclear
lesions thus result in symmetric, bilateral ptosis. Peripheral third nerve
deficits are much more common; they result from a wide variety of insults
including trauma, ischemia (microvascular disease), inflammation, neoplasm,
and aneurysms. Ptosis with decreased or absent levator function, pupillary
mydriasis, and paralytic strabismus typically are present. Spontaneous
recovery may occur, although a partial deficit often remains. Aberrant
regeneration is not infrequent and occasionally results in gaze-directed
eyelid retraction.
Repair of paralytic ptosis usually requires frontalis suspension. Surgery should be delayed for 6-12 months until it is certain that spontaneous recovery will not occur [28] . Coexisting strabismus should be corrected prior to ptosis repair, otherwise eyelid elevation may result in intractable diplopia.
Horner's syndrome
Muller's smooth muscle is sympathetically innervated and provides several
millimeters of eyelid elevation. Sympathetic denervation (Horner's syndrome)
results in moderate ptosis with preserved levator function (see Fig. 5.5)
. An abnormally high lower eyelid contributes to the narrowed palpebral
fissure, secondary to involvement of the inferior tarsal smooth muscle.
A relative ipsilateral miosis is uniformly present and many patients also
demonstrate hemifacial anhidrosis. Heterochromia may be noted in patients
who have congenital Horner's syndrome [29] in which the ipsilateral iris
is lighter in color.
Pharmacologic (cocaine) testing facilitates the diagnosis of this condition. The neurologic deficit may result from ischemia, trauma, neoplasm, or iatrogenic insults. A medical evaluation is indicated in patients with newly diagnosed Horner's syndrome without an apparent cause. The ptosis in acute cases should be observed. Surgical correction is indicated in patients who have significant, persistent disease.

Figure 5-4 Marcus Gunn' s jaw- winking syndrome. (a) In primary
gaze with the mouth closed, there is right upper eyelid ptosis. (b) With
the jaw opened the right upper eyelid elevates due to synkinesis.
--------------------------------------------------------------------------------
Section 7
5 . 4
![]() Figure 5-5 Horner' s syndrome
with ipsilateral right upper eyelid ptosis and pupillary miosis.
Figure 5-5 Horner' s syndrome
with ipsilateral right upper eyelid ptosis and pupillary miosis.
External levator aponeurotic-muscle resection or a posterior mullerectomy are effective methods of repair.
Myasthenia gravis
Ptosis or diplopia are the presenting symptoms in about one half of
patients who have myasthenia, and subsequently appear in 96% of all individuals
with this condition [30] . The ptosis may be unilateral, bilateral, or
alternating. Levator function is either decreased or variable. The affected
levator muscle usually demonstrates rapid fatigability, where the eyelid
twitches or slowly falls with prolonged upgaze [31] . This finding is distinct
from the increased ptosis associated with systemic fatigue, suffered by
all ptosis patients, irrespective of cause. A minority of myasthenic patients
maintain a purely ocular form of the disease, while the remainder develop
systemic involvement [32] [33] .
This autoimmunologic condition affects the function of the neuromuscular junction and has a predilection for muscles innervated by the cranial nerves. Antibodies to acetylcholine receptor protein are present in the majority of patients with systemic disease [32] . The history and clinical findings usually lead the clinician to the diagnosis, which is confirmed by Tensilon testing, electrophysiologic studies, or acetylcholine receptor antibody levels (Fig. 5.6) . Myasthenia is treated medically. Selected patients may benefit from thymectomy [33] . Ptosis repair is reserved for those individuals with refractory, visually debilitating disease. A limited frontalis suspension is usually performed. Myasthenia patients are at an increased risk for developing postoperative ocular exposure, secondary to coexisting orbicularis muscle weakness or a poor Bell's phenomenon.
Chronic progressive external ophthalmoplegia
Chronic progressive external ophthalmoplegia (CPEO) is a diffuse spectrum
of conditions which may either be hereditary or sporadic in nature. Most
patients present with symmetric, bilateral ptosis in early adulthood (Fig.
5.7) . The mitochondrial myopathy results in decreased levator function.
Extraocular muscles are later affected, resulting in diffuse ophthalmoplegia.
Associated systemic findings are present in some forms of this disease,
including cardiac conduction defects (Kearns-Sayre syndrome) and dysphagia
(oculopharyngeal dystrophy) [34] [35] [36] .
Muscle biopsy may be necessary to confirm the diagnosis of CPEO. Ptosis repair is typically deferred until the patient is visually debilitated. Limited frontalis suspension is usually the procedure of choice, avoiding postoperative lagophthalmos and resultant ocular exposure.
Aponeurotic redundancy or dehiscence
The majority of patients who have acquired ptosis develop the condition
secondary to involutional changes in the levator aponeurosis. A gradual
stretching or dehiscence of this structure occurs, which leads to a slowly
progressive ptosis. Chronic contact lens wearers also may develop ptosis
on this basis. Aponeurotic dehiscence suddenly may

Figure 5-6 Myasthenia gravis with severe bilateral ptosis. (a)
Before treatment. (b) The same patient after administration of intravenous
Tensilon.

Figure 5-7 Chronic progressive external ophthalmoplegia (CPEO)
with bilateral ptosis and ocular motility abnormality.
occur following ocular surgery or trauma. A significant ptosis develops in approximately 6% of patients following cataract surgery [37] .
Levator function remains excellent in this form of ptosis. Loss of the aponeurotic attachment results in an abnormally high or indistinct upper eyelid crease (Fig. 5.8) . The superior sulcus deepens and the upper eyelid may appear to be unusually thin, occasionally allowing visualization of the iris through the eyelid tissue. Surgical repair of the aponeurotic dehiscence effectively corrects the ptosis and is best performed with an anterior approach.
Mechanical ptosis
Mechanical ptosis may develop from cicatricial processes, orbital or
eyelid masses, or enophthalmos. Scarring involving any of the anatomic
layers of the upper eyelid or symblepharon between the lid and globe may
limit eyelid mobility and cause ptosis. Encapsulated orbital lesions may
alter levator function secondary to mass effect, while infiltrative conditions
restrict the muscle activity. The relative severity of mechanical ptosis
often varies in different gaze positions. Effective treatment of mechanical
ptosis requires correction of the underlying abnormality. Orbital mass
lesions may require surgery, radiation, or medical therapy.
--------------------------------------------------------------------------------
Section 7
5 . 5
Enophthalmos or phthisis alter the normal anatomic relationship between
the eye and upper eyelid. The loss of upper eyelid support from the recessed
globe results in ptosis and a smaller palpebral fissure. Enucleation or
the fitting of a scleral shell often improve ptosis in patients who have
phthisis. Restoration of the normal orbital volume usually reduces ptosis
in patients who have enophthalmos.
ALTERNATIVES TO SURGERY
Ptosis repair always is considered an elective procedure. Surgery should
be avoided or limited in individuals who have preoperative ocular irritation
or photophobia. Patients who have poor lacrimal production are at risk
for developing symptomatic dryness following eyelid elevation.

Figure 5-8 Levator function. (a) Bilateral ptosis from levator
aponeurosis dehiscence demonstrating a high indistinct lid crease. (b)
In upgaze, levator muscle function is of normal amplitude.( c) The indistinct
eyelid crease and ptosis remain in downgaze. (d) Normal lid height following
levator aponeurosis advancement.
Raising the ptotic eyelid of a patient who has an enlarged pupil or sector iridectomy may cause intractable light sensitivity. Individuals who have poor Bell's phenomena are at an increased risk for developing exposure keratitis, should postoperative lagophthalmos be present. Visually debilitating ptosis in the above patients can be repaired with limited surgery in an attempt to undercorrect the eyelid position. Nonsurgical elevation of the eyelid with a ptosis crutch attached to the spectacle frame can occasionally be helpful, although these devices usually limit the blink, which often results in ocular irritation.
ANESTHESIA
Ptosis repair ideally is performed under local infiltrative anesthesia.
An alert, awake patient facilitates the intraoperative adjustment of eyelid
position and contour. The subcutaneous injection of a mixture of 2% lidocaine
(lignocaine) with 1:200,000 epinephrine (adrenaline) and 0.75% bupivacaine
provides adequate intraoperative and postoperative analgesia. A minimal
volume (1-2cm3 per eyelid) of anesthetic is required. Larger volumes or
deeper orbital injections may alter levator function, which compromises
muscle adjustment. General anesthesia is necessary for young children,
certain apprehensive adults, and when harvesting autologous fascia lata.
GENERAL TECHNIQUES
The type of ptosis and amount of levator function determine which procedure
to perform. Patients who have moderate-good levator function have their
disorder effectively corrected with an anterior levator aponeurotic-muscle
reattachment or resection. This same procedure may be employed in cases
with poor levator activity, although large resections are necessary, which
result in postoperative lagophthalmos. Some surgeons perform a posterior
resection of Muller's muscle in patients who demonstrate adequate elevation
of the eyelid following instillation of topical phenylephrine. [38] [39]
Frontalis suspension often is the procedure of choice in patients who show severe ptosis, poor levator activity, and intact frontalis muscle function. Autologous fascia lata remains the preferred implant material in pediatric cases. Preserved donor fascia is available, although absorption with subsequent recurrent ptosis may occur [40] . Silicone rods often are employed in patients in whom it is impractical to harvest fascia lata. Alloplastic implants occasionally are complicated by extrusion, infection, or breakage.
The quality of the Bell's phenomenon, lacrimal production, and orbicularis activity are all considered when determining the amount of eyelid elevation that is ideal in each case of ptosis repair. Selected patients tolerate mild lagophthalmos, which may be necessary to achieve an acceptable cosmetic result in those who have severe congenital ptosis. Marked lagophthalmos generally should be avoided, due to the risks of early or chronic corneal exposure.
The upper eyelid skin incision usually is placed in the location of the desired eyelid crease. The position of the uninvolved eyelid's crease is matched in cases of unilateral ptosis. The creases often are absent or indistinct in cases of severe, bilateral disease. The normal crease is usually positioned one third of the distance from the eyelashes to the lower edge of the brow, measured in downgaze [41] . The central incision is approximately 9-10mm above the lashes in adult women. The adult male crease is usually placed 1-2mm lower. Dermatochalasis can be simultaneously corrected in older patients who undergo bilateral ptosis repair. Redundant skin is excised from above the eyelid crease incision prior to elevating the eyelid.
Occasionally, children who show severe congenital ptosis are at risk
for developing occlusion amblyopia. Early surgical intervention may be
indicated in these individuals. Ptosis repair in young children is otherwise
deferred until 3 to 5 years of age, allowing maturation of the eyelid and
facilitating both preoperative measurements and postoperative care. It
is difficult to obtain sufficient fascia lata in children less than 3 years
of age.
--------------------------------------------------------------------------------
Section 7
5 . 6
SPECIFIC TECHNIQUES
Anterior levator aponeurosis advancement
Immediately prior to surgery the patient is examined while sitting
and supine. Any variation in eyelid position is noted, since the eyelid
adjustment will be performed while the patient is recumbent. A standard
full-face surgical wash is performed to allow intraoperative comparison
of both orbits. The desired position of the upper eyelid crease incision
is marked on the ptotic eyelid(s). Subcutaneous infiltrative anesthesia
is administered.
The incision is created with a scalpel blade ( Fig. 5.9a ). Sharp-tipped Westcott scissors may be employed for the remaining dissection. The fine subcutaneous tissue is divided to expose the underlying orbicularis muscle (see Chapter 7 .1). A buttonhole is cut through the center of the muscle and the layer is incised medially and laterally parallel to the muscle fibers. Hemostasis is maintained throughout the procedure with bipolar, wetfield cautery. The orbital septum and underlying orbital fat usually are visible at this point. Superior retraction of these structures may occur in cases of marked aponeurotic dehiscence. The septum is divided and the preaponeurotic fat pads are retracted upward to expose the underlying levator muscle ( Fig. 5.9b ).
The opaque levator aponeurosis may be very thin and stretched or completely dehisced from its tarsal attachments. The conscious patient is now asked to open his or her eyes to allow the surgeon to determine if the surgical dissection has altered the preoperative eyelid level. Any remaining distal attachments of the aponeurosis are divided, exposing the tarsus. The aponeurosis is separated from the underlying Muller's muscle using both blunt and sharp dissection ( Fig. 5.9c ). In patients who have marked attenuation of the aponeurosis, such as in severe congenital ptosis, the combined aponeurosis-Muller's muscle complex may have to be advanced as a unit to achieve adequate lid elevation. The dissection in these cases is performed between Muller's muscle and conjunctiva.
Several interrupted 6-0 polyester (Mersilene) sutures are placed through partial thickness of the tarsus medially, centrally, and laterally. The surgeon must examine the posterior surface of the lid to insure these sutures are not exposed on the conjunctiva. These sutures are used to reattach or advance the aponeurosis ( Fig. 5.9d ). Multiple adjustments may be needed to achieve the appropriate eyelid position and contour, and compensate for any alteration of lid position that may have been noted either when the patient was placed supine or during the surgical dissection. The eyelid level is adjusted empirically in patients under general anesthesia, considering the preoperative levator function and severity of disease. Redundant aponeurotic tissue is excised. It is advisable to recreate the eyelid crease by suturing the cut edge of either the pretarsal orbicularis muscle or subcutaneous tissue to the aponeurosis with interrupted 7-0 polyglactin (Vicryl) sutures ( Fig. 5.9e ). The skin incision is closed with a running 7-0 polypropylene (Prolene) suture ( Fig. 5.9f ).
Patients are observed for 30-60 minutes following surgery to detect early postoperative hemorrhage or other complications. Cold compresses may be applied while awake for the first 48 hours to minimize edema and ecchymosis. Subsequent wet and warm compresses assist in wound hygiene. A topical antibiotic ointment is placed on the incision several times daily. Suture removal is performed 5-7 days following surgery. Mild lagophthalmos and poor blink often are noted in the early postoperative period, even in appropriately positioned eyelids. This finding may be attributable to orbicularis underaction, which typically improves several weeks after surgery. A variable period of time is required for complete resolution of the postoperative edema and stabilization of the eyelid level.
Frontalis suspension
The pattern of frontalis action, whether diffuse or segmental, is noted
prior to surgery. The availability of suspensory material and the brow
contour dictate the incision location and the pattern of threading the
implanted sling. Common implant materials include autologous fascia lata
and silicone rods. The usual patterns for threading these materials are
either in one continuous pentagonal polygon or with a triangular sling.
A pentagonal-shaped sling usually is placed in patients who have diffuse
brow elevation. Medial and lateral horizontal incisions are marked at the
superior border of the brow. A central forehead incision
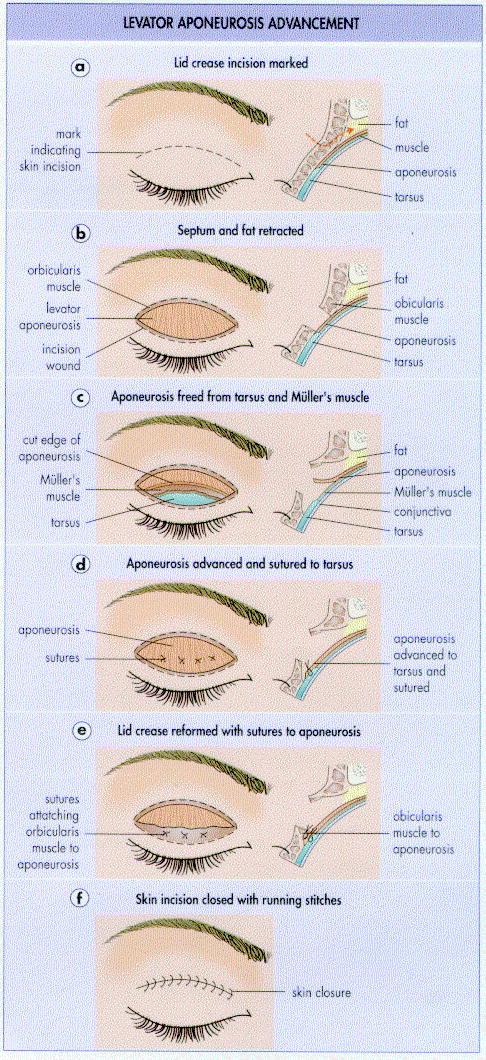
Figure 5-9 Key steps in levator aponeurosis advancement.
--------------------------------------------------------------------------------
Section 7
5 . 7
is placed approximately 10mm above the brow and between the other two
incisions. Triangular slings may be more ideal in individuals who have
segmental brow elevation, as they utilize a single incision above the area
of the brow that exhibits maximal movement.
Regardless of the sling configuration, brow stab incisions are cut through the skin and subcutaneous tissue, exposing the frontalis muscle in the appropriate locations. Generally, these are located just outside the medial and lateral corneal limbus ( Fig. 5.10a ). A crease incision is created in the eyelid. The subcutaneous tissue, orbicularis muscle, and orbital septum are opened in separate layers ( Fig. 5.10b ). The anterior surface of the tarsus is exposed and hemostasis achieved with bipolar, wetfield cautery.
Fascia lata next must be harvested in patients who undergo autologous grafting. A 3cm incision is made on the lower thigh, just above the lateral condyle of the femur. The white, glistening fascia lata is visible underneath the subcutaneous fat. Blunt dissection is performed along the anterior surface of the fascia, up the lateral aspect of the leg for about 15-20cm. A strip of fascia 6-8mm wide and 15-20cm long is harvested using fascial stripper and cutter. The fascia is cleaned of adherent subcutaneous fat and divided into 2-3mm wide strips.
The autologous fascia or alloplastic implant material (silicone rods, permanent sutures) is sutured to the upper anterior surface of the central tarsus with several partial thickness 6-0 polyester sutures ( Fig. 5.10c ). Eyelid contour can be adjusted by altering the width of this attachment. A Wright fascial needle is then used to pass each end of the sling material first through the peripheral brow incisions and then from these to the central brow incision. The implant is positioned deep to the orbital septum within the lid and superficial to the periosteum over the superior orbital rim. It is best to recreate the eyelid crease by suturing the edge of the pretarsal orbicularis muscle to the aponeurosis with 7-0 polyglactin sutures. The eyelid crease incision is then closed with 7-0 polypropylene in adults or 7-0 chromic sutures in children prior to adjusting the eyelid height ( Fig. 5.10d ). Tensions on the two ends of the sling are adjusted by pulling up on the free ends together at the central brow incision in order to achieve the proper lid height and contour. The ends then are joined with either permanent sutures (fascia) or a silicone sleeve (silicone rods), prior to being buried underneath the subcutaneous tissue of the forehead. The brow and leg incisions are closed in a layered fashion. A light elastic leg dressing may minimize the risk of postoperative hematoma. Postoperative wound care is similar to the regimen described for anterior levator surgery.
COMPLICATIONS
Successful ptosis repair requires a complete understanding of the surgical
anatomy and function of the upper eyelid. Meticulous surgical technique
minimizes the occurrence of many surgical complications, such as hemorrhage,
infection, poor wound healing, and visual loss. Excessive dissection of
the levator may traumatize the superior oblique muscle or lacrimal gland
ductules. Appropriate preoperative evaluation and patient selection reduce
the risks of postoperative ocular irritation, keratitis, and photophobia.
Undercorrection
Persistence of some postoperative eyelid droopiness is the most common
complication of ptosis repair, seen in about 10-15% of patients. These
patients should be observed until the surgeon is certain that all edema
has resolved and the eyelid position has stabilized. In some cases a surgical
revision is needed to obtain an ideal position of the eyelid. Further levator
resection or brow suspension may limit lid closure in some patients. An
unsuspected acquired myopathy may be responsible for recurrent or poorly
corrected ptosis. Such patients may require repeated ptosis correction
over many years.
Overcorrection
Patients who have mild overcorrection following ptosis repair also
should be observed until the lid position has become stable. Digital massage
or 'squeezing' exercises occasionally provide a slight lowering of the
eyelid, which improves mild overcorrection. Surgical revision with recession
of the levator or suspension material is indicated in cases with persistent
overcorrection. Emergent, early surgical revision should be performed in
patients who show marked postoperative overcorrection and ocular exposure.
![]()
Figure 5-10 Key steps in frontalis suspension.
--------------------------------------------------------------------------------
Section 7
5 . 8
Eyelid crease abnormalities
Incorrect incision planning or failure to adequately create the eyelid
crease may result in either an indistinct or a poorly positioned crease.
An absent or abnormally low crease may be reformed by placing an incision
through skin and orbicularis muscle in the location of the new crease.
The subcutaneous tissue or orbicularis muscle is sutured to the aponeurosis,
prior to skin closure.
It is very difficult to lower an abnormally high crease. The attachment between the skin-orbicularis muscle and the aponeurosis must be separated. Soft tissue, such as orbital fat, then should be mobilized between these layers, in an effort to minimize the establishment of a new adhesion in the same location. The new crease then is established at a lower level.
Abnormalities of eyelid margin contour
Distortions of the eyelid margin contour result from uneven advancement
of the aponeurosis. If mild, segmental massage of the higher portion may
be helpful. However, in many cases a surgical revision is required, with
tightening or loosening of individual sutures. This often can be accomplished
at the 1-week follow-up visit, before the skin wound flaps are firmly united.
Lagophthalmos and exposure keratitis
Keratitis following ptosis repair may be related to overcorrection,
lagophthalmos, inadequate blink, decreased tear production, or a poor Bell's
phenomenon. Nighttime lubricating ointment and topical artificial tears
are employed to treat minor cases. Bandage soft contact lenses occasionally
can be helpful. Punctal occlusion may be indicated in patients who have
severe dry eyes. Persistent keratitis in patients who have poor blink or
lagophthalmos may require lowering of the upper eyelid. Alternative procedures,
such as elevating the lower lid, canthoplasty, and tarsorrhaphy, can be
considered for patients in whom reversal of the ptosis repair would be
visually disabling.
Prolapse of the superior conjunctival fornix
With excessive advancement of the aponeurosis or Muller's muscle the
superior conjunctiva may prolapse into the palpebral fissure. This results
from failure to separate the fine attachments between the aponeurosis and
the superior fornix suspensory ligaments. If the conjunctival is easily
reduced, a pressure patch for several days may correct the condition. Once
fibrosis supervenes, direct excision is necessary.
OUTCOME
The vast majority of ptosis procedures are successful and restore a
normally functioning eyelid and improve superior visual field. The new
eyelid position usually remains stable, with recurrences being uncommon.
Patients who have congenital ptosis, acquired myopathies, or postoperative
lagophthalmos require continued evaluation after surgery to detect possible
ocular exposure or the development of associated ophthalmic conditions.
REFERENCES
1. Motais M. Operation du ptosis par la greffe tarsienne d'une languette du tendon du muscle droit superieur. Ann Oculist (Paris). 1897;118:5-12.
2. Parinaud H. Nouveau procede operatoire dy ptosis. Ann Oculist (Paris). 1897;118:13-17.
3. Bader. Report of the chief operations performed at the Royal London Ophthalmic Hospital for quarter ending 25th September 1857. Royal London Ophthalmic Hosp Rep. 1857;1:33-5.
4. Beard CH. Ophthalmic surgery, 2nd edn. Philadelphia: P Blakiston's and Sons Co; 1914:230-52.
5. Eversbusch O. Zur operation der congenitalen blepharoptosis. Klin Monatsbl Augenheilkd. 1883;21:100-7.
6. Jones LT, Quickert MH, Wobig JL. The cure of ptosis by aponeurotic repair. Arch Ophthalmol. 1975;93:629-34.
7. Gay AJ, Salmon ML, Windsor CE. Hering's law, the levators, and their relationship in disease states. Arch Ophthalmol. 1967;77:157-60.
8. Schechter RJ. Ptosis with contralateral lid retraction due to excessive innervation of the levator palpebrae superioris. Ann Ophthalmol. 1978;10:1324-8.
9. Fox SA. The palpebral fissure. Am J Ophthalmol. 1966;62:73-8.
10. Smith B, McCord CD, Baylis H. Surgical treatment of blepharoptosis. Am J Ophthalmol. 1969;68:92-9.
11. Anderson RL, Baumgartner SA. Strabismus in ptosis. Arch Ophthalmol. 1980;98:1062-7.
12. Berke RN. Congenital ptosis - a classification of two hundred cases. Arch Ophthalmol. 1948;41:188-97.
13. Carbajal UM. An analysis of 142 cases of ptosis. Am J Ophthalmol. 1958;45:692-704.
14. Sevel D. Ptosis and underaction of the superior rectus muscle. Ophthalmology. 1984;91:1080-5.
15. Beneish R, Williams F, Polomeno RC, et al. Unilateral congenital ptosis and amblyopia. Can J Ophthalmol. 1983;18:127-30.
16. Merriam WW, Ellis FD, Helveston EM. Congenital blepharoptosis, anisometropia, and amblyopia. Am J Ophthalmol. 1980;89:401-7.
17. Anderson RL, Baumgartner SA. Amblyopia in ptosis. Arch Ophthalmol. 1980;98:1068-9.
18. Callahan A. Surgical correction of the blepharophimosis syndromes. Trans Am Acad Ophthalmol Otolaryngol. 1973;77:op687-op695.
19. Briggs HH. Hereditary congenital ptosis with report of 64 cases conforming to the Mendelian rule of dominance. Am J Ophthalmol. 1919;2:408-17.
20. Townes PL, Muechler EK. Blepharophimosis, ptosis, epicanthus inversus, and primary amenorrhea - a dominant trait. Arch Ophthalmol. 1979;97:1664-6.
21. Mustarde JC. Experiences in ptosis correction. Trans Am Acad Ophthalmol Otolaryngol. 1968;72:173-85.
22. Gunn RM. Congenital ptosis with peculiar associated movements of the affected lid. Trans Ophthalmol Soc UK. 1883;3:283-5.
23. Oesterle CS, Faulkner WJ, Clay R, et al. Eye bobbing associated with jaw movement. Ophthalmology. 1982;89:63-7.
24. Lewy FH, Groff RA, Grant FC. Autonomic innervation of the eyelids and the Marcus Gunn phenomenon. Arch Neurol Psychiatr. 1937;37:1289-97.
25. Spaeth EB. The Marcus Gunn phenomenon. Am J Ophthalmol. 1947;30:43-158.
26. Pratt SG, Beyer CK, Johnson CC. The Marcus Gunn phenomenon (a review of 71 cases). Ophthalmology. 1984;91:27-30.
27. Bullock JD. Marcus Gunn jaw-winking ptosis: classification and surgical management. J Pediatr Ophthalmol Strabismus. 1980;17:375-9.
28. Krohel GB. Blepharoptosis after traumatic third-nerve palsies. Am J Ophthalmol. 1979;88:598-601.
29. Weinstein JM, Zweifel TJ, Thompson HS. Congenital Horner's syndrome. Arch Ophthalmol. 1980;98:1074-8.
30. Mattis RD. Ocular manifestations in myasthenia gravis. Arch Ophthalmol. 1941;26:969-82.
31. Cogan DG. Myasthenia gravis. Arch Ophthalmol. 1965;74:217-21.
32. Oasterhuis HJ. The ocular signs and symptoms of myasthenia gravis. Doc Ophthalmol. 1982;52:363-78.
33. Seybold ME. Myasthenia gravis. A clinical and basic science review. JAMA. 1983;250:2516-21.
34. Duranceau AC, Beauchamp G, Jamiewon GG, et al. Oropharyngeal dysphagia and oculopharyngeal muscular dystrophy. Surg Clin North Am. 1983;63:825-32.
35. Johnson CC, Kuwabara T. Oculopharyngeal muscular dystrophy. Am J Ophthalmol. 1974;77:872-9.
36. Bastiaenson LA, Frenken CW, TerLaak HJ, et al. Kearns syndrome: A heterogeneous group of disorders with CPEO, or a nasological entity? Doc Ophthalmol. 1982;52:207-25.
37. Feibel RM, Custer PL, Gordon MO. Postcataract ptosis - a randomized, double-masked comparison of peribulbar and retrobulbar anesthesia. Ophthalmology. 1993;100:660-5.
38. Putterman AM. Muller muscle-conjunctiva resection - technique for treatment of blepharoptosis. Arch Ophthalmol. 1975;93:619-23.
39. Weinstein GS, Buerger GF. Modifications of the Muller's muscle-conjunctival resection operation for blepharoptosis. Am J Ophthalmol. 1982;93:647-51.
40. Crawford JS. Recent trends in ptosis surgery. Ann Ophthalmol. 1975;7:1263-7.
41. Zamora RL, Becker WL, Custer PL. Normal eyelid crease position in
children. Ophthalmic Surg. 1993:25:42-7.
--------------------------------------------------------------------------------
MD Consult L.L.C. http://www.mdconsult.com
Bookmark URL: /das/book/view/899/94.html/top